‹ Subcostal four chamber view
Importance of subcostal views
Subcostal views are ideal in a lot of clinical situations, like assessing pericardial effusion, having a quick look at the cardiac function on the intensive care unit, looking for the presence of an ASD or assessing a patient's inferior vena cava. In a lot of textbooks, it is said that the subcostal views are really easy to acquire and that even novices don't have any problems getting these views. Unfortunately, that is not what it is like in the real world. You have to practice these views like any other, to avoid foreshortening, off-axis scanning or similar problems. Giving the patient breathing commands can help a lot to get the best out of an image.

An indisputable advantage of the subcostal views is that the patient can lie on his back and even ventilated patients who can not be moved can be scanned.
Echocardiography
Visible structures
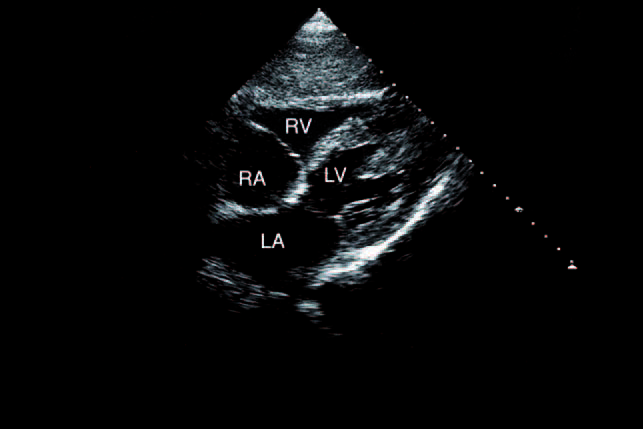
In the subcostal four chamber view, one can get an excellent overview of many heart structures: the right ventricle (RV), the right atrium (RA), the left atrium (LA), the left ventricle (LV), the atrioventricular valves and the pericardial space.
Please note that the right ventricular wall visible in this view is not the same you see when acquiring an apical four chamber view. The apical four chamber view displays the free lateral right ventricular wall, while in the subcostal view the inferior right ventricular wall can be seen.
When the image looks like the one above, the index of the transducer points toward the left side of the patient. This puts the liver at the top of the image and the heart below.
The subcostal view is also excellent to scan for pericardial effusion and describe its circumferential extend.
An example of a control patient with normal findings.
Tip
To reduce the tension of the abdominal muscles, the patient should bend his knees while lying on the back.
What else is important?
Especially in patients which are quite cumbersome to scan from the parasternal and apical position, the subcostal view can be used to assess left ventricular chamber size and function, although a direct ejection fraction calculation should not be done using the subcostal views.
Colour Doppler can be used to scan for atrial or ventricular septal defects. This is very useful as the orientation of the interventricular and atrial septum is almost perpendicular to the axis of the transducer and thus, shunts head almost parallel to the beam axis.
Right ventricular hypertrophy is assessed using the subcostal four chamber view. This can be down via m-mode or 2D. A wall thickness of the inferior wall of more than 5 mm is considered to define right ventricular hypertrophy.